Preoperative Lung nodule localization using Hookwire, an approach to early diagnosis and treatment of Lung cancer - Literature review and case series report
Abstract
In clinical practice of respiratory diseases, we often encounter solitary pulmonary nodules (SPN). SPNs have 3 main forms: (1) Solid nodules (SN); (2) Part-solid nodules (PS); (3) Ground glass opacity (GGO); (4) Cyst nodules (CN). There have been many guidelines from different societies/society around the world on the management of SPN (NCCN; Fleischner; ATS; ERS...). However, these instructions are general and do not address the issue of individualization. To be able to treat/cure lung cancer well, early detection and choosing appropriate treatment methods play a decisive role. Association guidelines are based on size, structure, and risk factors to devise a management strategy for solitary nodules, which factors in nodule size at first detection as well as subsequent screenings, play a key role. According to NCCN: (1) SN, ≥ 8mm
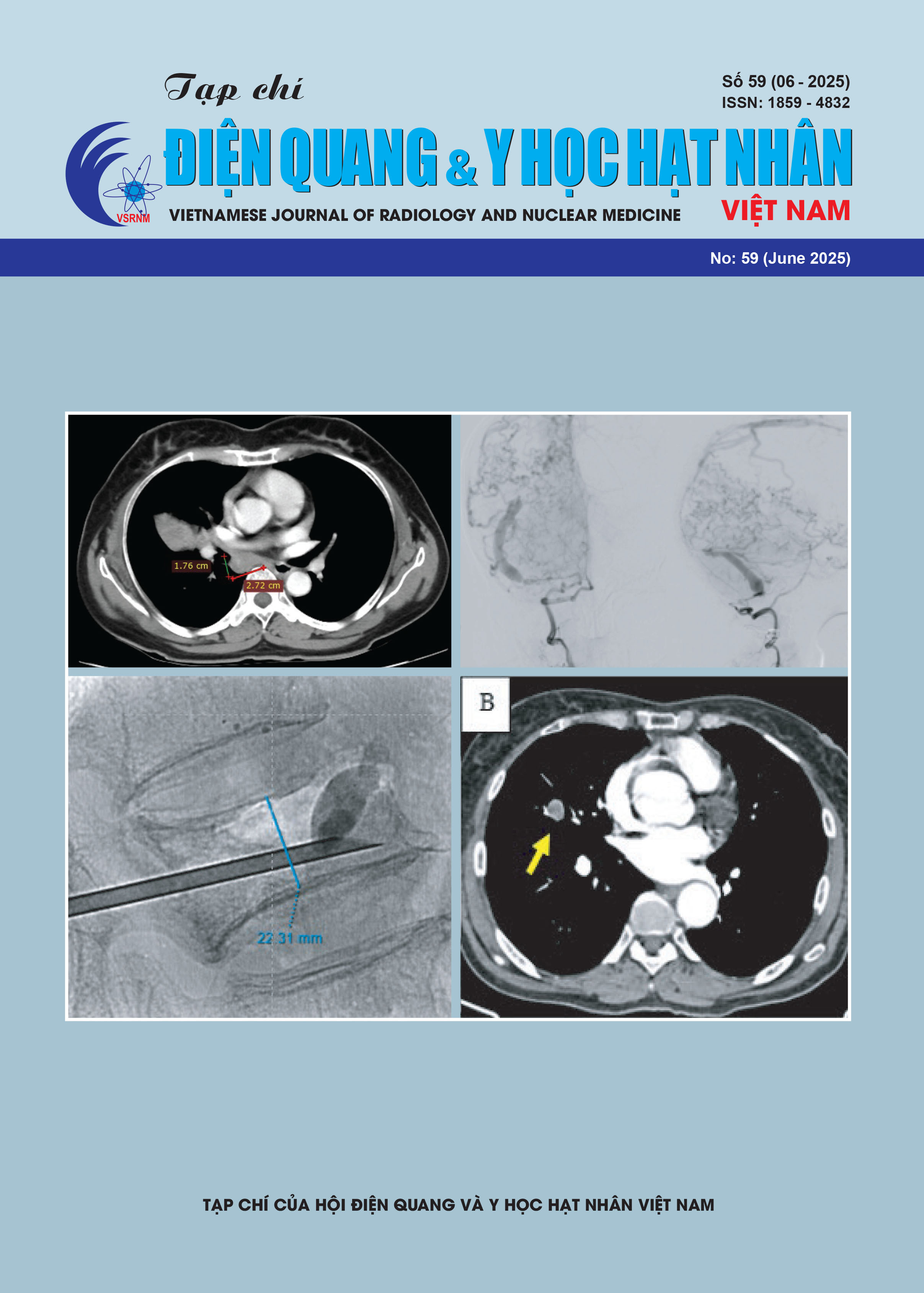
to > 15 mm in subjects at high risk of lung cancer should be monitored by LDCT every 3 months or PET scan; Nodules ≥ 15 mm should have a contrast CT scan/PET scan/tissue sampling. If the results indicate high suspicion of LC, the biopsy/nodular excision is indicated; (2) PS nodules when the solid part is ≥ 8mm, at high risk subjects can be applied above techniques; (3) GGO < 20 mm, monitoring by LDCT once a year; > 20 mm every 6 months, no recommendation for biopsy or resection. Thus, if this recommendation is applied correctly, there will be many cancerous nodules under the above sizes that will be "nourished" until they meet treatment standards, which will inevitably reduce the chance of being diagnosed and receiving early treatment, losing the opportunity to "cure" the patient. Another common situation: A single nodule/mass on one side of the lung is still amenable to surgery, but another single nodule appears in the same lung on the same side but in a different lobe or on the opposite lung. So, very important to confirm the nodule is secondary/non-secondary before lobectomy containing the primary lesion. In this situation, according to our knowledge, there is no guideline for recommendation. We report 22 cases in which lung nodules were located before thoracoscopic surgery (VAST) using Hookwire, many of which were assigned an "individualized" approach (not a recommendation) and gave surprising results. The discussion is based on an analysis of image characteristics and pathological results and recommends the idea of "individualizing" each case for colleagues to refer to.